Neoplasms, Multiple Primary
Neoplasms, Second Primary
Adenomatosis, Pulmonary
Germ-Line Mutation
Li-Fraumeni Syndrome
Paget's Disease, Mammary
Melanoma
Neoplastic Syndromes, Hereditary
Gastrointestinal Neoplasms
Genes, p16
Soft Tissue Neoplasms
Genes, p53
Osteosarcoma
Registries
Sarcoma
Pedigree
Genetic Predisposition to Disease
Head and Neck Neoplasms
Carcinoma, Squamous Cell
Pancreatic Neoplasms
Risk
Incidence
Neoplasms
Prognosis
Mutation
Neoplasm Staging
Neoplasms, Cystic, Mucinous, and Serous
Exons
Retrospective Studies
Risk Factors
Tumor Suppressor Protein p53
Follow-Up Studies
Merkel cell carcinoma and melanoma: etiological similarities and differences. (1/1469)
Merkel cell carcinoma (MCC) of the skin and cutaneous malignant melanoma can now be compared epidemiologically through the use of population-based data not previously available for MCC. The results may provide new clues to etiology. In this study, United States data covered by the Surveillance, Epidemiology, and End Results (SEER) Program were from nine areas of the United States (approximately 10% of the population). In 1986-1994, 425 cases of MCC were registered. The annual age-adjusted incidence per 100,000 of MCC was 0.23 for whites and 0.01 for blacks; among whites, the ratio of melanoma to MCC was approximately 65 to 1. Only 5% of MCC occurred before age 50, unlike the lifelong risk of nodular and superficial spreading melanoma. Regional incidence rates of both cancers increased similarly with increasing sun exposure as measured by the UVB solar index. The most sun-exposed anatomical site, the face, was the location of 36% of MCC but only 14% of melanoma. Both cancers increased in frequency and aggressiveness after immunosuppression and organ transplantation (36 cases from the Cincinnati Transplant Tumor registry and 12 from published case reports) and after B-cell neoplasia (5 cases in this study; 13 from case series in the literature). The SEER data contained reports of six patients with both types of cancer; 5 melanomas before the diagnosis of MCC and 1 after diagnosis. MCC and melanoma are similarly related to sun exposure and immunosuppression, but they differ markedly from one another in their distributions by age, race, and anatomical site, especially the face. (+info)The elevated serum alkaline phosphatase--the chase that led to two endocrinopathies and one possible unifying diagnosis. (2/1469)
A 39-year-old Chinese man with hypertension being evaluated for elevated serum alkaline phosphatase (SAP) levels was found to have an incidental right adrenal mass. The radiological features were characteristic of a large adrenal myelolipoma. This mass was resected and the diagnosis confirmed pathologically. His blood pressure normalised after removal of the myelolipoma, suggesting that the frequently observed association between myelolipomas and hypertension may not be entirely coincidental. Persistent elevation of the SAP levels and the discovery of hypercalcaemia after surgery led to further investigations which confirmed primary hyperparathyroidism due to a parathyroid adenoma. The patient's serum biochemistry normalised after removal of the adenoma. The association of adrenal myelolipoma with primary hyperparathyroidism has been reported in the literature only once previously. Although unconfirmed by genetic studies this association may possibly represent an unusual variation of the multiple endocrine neoplasia type 1 syndrome. (+info)A case of long-term survival with stage IV small cell lung cancer and early-stage central-type squamous cell lung cancer treated by photodynamic therapy. (3/1469)
The present report is on a 67-year-old man with stage IV small cell lung cancer and early-stage centrally located squamous cell cancer of the lung. He was diagnosed as small cell lung cancer with multiple metastasis to the ipsilateral lung and was found to have a central-type early-stage squamous cell cancer by bronchoscope. After obtaining a complete response to the small cell lung cancer with chemotherapy and radiotherapy, photodynamic therapy was applied to the squamous cell carcinoma, resulting in complete disappearance of the tumor. Recurrence of small cell cancer occurred at the ipsilateral lung and this patient died of small cell cancer 8 years after initiation of treatment. Post mortem examination confirmed complete disappearance of squamous cell cancer treated by photodynamic therapy. This is a rare case of long-term survival with stage IV small cell lung cancer and early-stage central-type squamous cell lung cancer successfully treated by photodynamic therapy. (+info)p53 and p16INK4A mutations during the progression of glomus tumor. (4/1469)
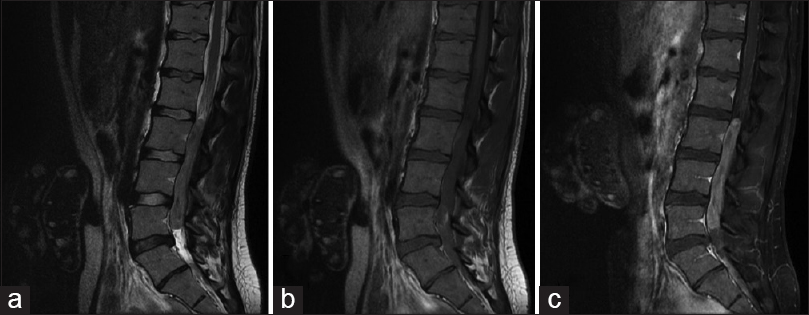
Glomus tumors are significantly rare tumors of carotid body. The great majority of these tumors are benign in character. Here we present two brothers with hereditary glomus jugulare tumor who had consanguineous parents. Radiotherapy was applied approximately 8 and 10 years ago for treatment in both cases. Eight years later, one of these cases came to our notice due to relapse. The mutation pattern of p53, p57KIP2, p16INK4A and p15NK4B genes which have roles in the cell cycle, was analyzed in tumor samples obtained from the two affected cases in the initial phase and from one of these cases at relapse. The DNA sample obtained from the case in initial diagnosis phase revealed no p53, p57KIP2, p16INK4A or p15INK4B mutation. He is still in remission phase. Despite the lack of p53, p57KIP2, p16INK4A and p15INK4B mutation at initial diagnosis the tumor DNA of the other case in relapse revealed p53 codon 243 (ATG-->ATC; met-->ile) and p16 codon 97 (GAC-->AAC; asp-->asn) missense point mutations. No loss of heterozygosity in p53 and p16INK4A was observed by microsatellite analysis of tumoral tissues in these cases. P53 and p16INK4A mutations observed in relapse phase were in conserved regions of both genes. No previous reports have been published with these mutations in glomus tumor during progression. The mutation observed in this case may due to radiotherapy. In spite of this possibility, the missense point mutations in conserved region of p53 and p16INK4A genes may indicate the role of p53 and p16INK4A in tumor progression of glomus tumors. (+info)Primary endometrioid carcinoma of fallopian tube. Clinicomorphologic study. (5/1469)
Twenty cases of primary Fallopian tube endometrioid carcinoma (PFTEC) are presented in the paper. This accounts for 42.5% of all histologic forms of primary Fallopian tube carcinoma (PFTC) found in our Department. The youngest patient was 38, and the oldest 68 years (mean: 56 years). Seven patients were nulliparas. Only two cases were bilateral. According to FIGO staging, 13 cases were evaluated as stage I, 4 as II, and 3 as stage III. Due to the histologic grading, 8 tumors were classified as well, 7 as moderately, and 5 as poorly differentiated. In the time of preparation of the manuscript, 12 women were still alive, 2 of them with recurrent disease. The follow-up of patients without recurrence ranged from 4 to 120 months (median: 63). Eight patients had died (survival time: from 4 to 65 months; median: 26). Metastases were found in 8 patients, especially to ovaries. In 14/20 cases of PFTEC various forms of tubal wall invasion were observed. Blood or lymphatic vessels involvement was found in 9 patients. Six of them had died and one is alive with the symptoms of disease. Immunohistochemical detection of the mutant form of p53 protein and oncogene product, c-erbB-2, was studied in 17 cases. Nine patients exhibited simultaneous p53 protein accumulation and c-erbB-2 expression. 2/9 of these patients are alive with recurrent tumors and 4/9 died. Endometrioid carcinoma of the Fallopian tube can be characterized by a tendency to superficial invasion of tubal wall and in a half of the cases by invasion of vessels. The majority of these tumors were diagnosed at an early stage tumors. (+info)Epidemiological analysis of site relationships of synchronous and metachronous multiple primary cancers in the National Cancer Center, Japan, 1962-1996. (6/1469)
BACKGROUND: Multiple primary cancer (MPC) has been recognized as a problem commonly encountered in routine medical practice. A study of MPC is necessary not only to provide insights into the etiology of cancer, but also to provide information for effective medical care by clinical oncologists. METHODS: A cohort of 49,751 cancer patients who were admitted to the National Cancer Center Hospital between 1962 and 1996 was used to study the site relationship of MPC. Logistic and Poisson regression analyses using an internal reference group within the cohort were applied for the calculation of the prevalence odds ratio (POR) for site relationships of synchronous MPC and the incidence rate ratio (IRR) for those of metachronous MPC. RESULTS: Three site combinations with elevated risks for both synchronous and metachronous MPCs, eight with elevated risk for synchronous MPC, five with elevated risk for metachronous MPC and six with decreased risk for synchronous MPC were identified with statistical significance. Among them, the increased risk of metachronous stomach cancer following lymphoma and myeoloma (POR = 1.0 and 1.1, P > 0.05; IRR = 2.5, P < 0.05) and the inverse site-correlation of synchronous MPC between [trachea, bronchus and lung] and other sites of the upper aerodigestive tract [lip, oral cavity and pharynx] (POR = 0.5 and 0.3, P < 0.05) and esophagus (POR = 0.7 and 0.3, P < 0.05) have not been reported previously. CONCLUSIONS: Our results suggest that interventions for lymphoma and myeloma might affect the development of subsequent stomach cancer and additional etiological factors other than tobacco smoking are associated with the development of cancer in the upper aerodigestive tract. (+info)Discrimination of double primary lung cancer from intrapulmonary metastasis by p53 gene mutation. (7/1469)
When multiple synchronous lung tumours are identified, discrimination of multicentric lung cancers from intrapulmonary metastases by clinical findings is often difficult. We used genetic alterations in p53 gene as a discrimination marker of double primary lung cancers from single lung cancer with intrapulmonary metastasis. Twenty of 861 patients with primary lung cancer who underwent lung resection were selected as subjects because they showed synchronous double solid tumours of the same histological type in the unilateral lung without distant metastases. In addition, they had been diagnosed as lung carcinoma with intrapulmonary metastasis by clinical and histological findings. DNAs were extracted from paraffin-embedded tissue of paired tumours from these 20 patients. Exons 5-9 of the p53 gene were examined for genetic alterations in the tumours by polymerase chain reaction, single-strand conformation polymorphism analysis and subsequent DNA sequencing analysis. Three different patterns in the distribution of p53 mutations in double lung tumours were observed: [A] mutation in only one of the tumours (four cases), [B] different mutations in the tumours (two cases), and [C] same mutation in both tumours (one case). The cases of [A] or [B] patterns could be classified as double primary lung cancers, while the case of the [C] pattern was suggested to be lung cancer with intrapulmonary metastasis. These results suggested that the multicentric cancers were more frequent than the intrapulmonary metastatic cancers in double cancer cases. (+info)Mismatch repair gene defects contribute to the genetic basis of double primary cancers of the colorectum and endometrium. (8/1469)
Hereditary non-polyposis colorectal cancer (HNPCC) is a dominantly inherited cancer syndrome caused by germline defects of mismatch repair (MMR) genes. Endometrial cancer is the most common extracolonic neoplasm in HNPCC and is the primary clinical manifestation of the syndrome in some families. The cumulative incidence of endometrial cancer among HNPCC mutation carriers is high, estimated to be from 22 to 43%. We hypothesized that women with double primary cancers of the colorectum and endometrium are likely to be members of HNPCC families. In order to determine how frequently HNPCC manifests in the context of double primary cancers, we examined alterations of two MMR genes, hMSH2 and hMLH1, in 40 unrelated women affected with double primary cancers. These cases were identified using hospital-based and population-based cancer registries in Ontario, Canada. MMR gene mutations were screened by single-strand conformation polymorphism analysis and confirmed by direct sequencing. Eighteen percent (seven of 40) were found to harbor mutations of one of the two MMR genes. Analysis of colorectal and/or endometrial tumors of mutation-negative probands found microsatellite instability in seven of 20 cases. Six of seven mutation-positive probands had strong family histories suggestive of HNPCC. First degree relatives of mutation-positive probands had a very high relative risk (RR) of colorectal cancer (RR = 8.1, CI 3. 5-15.9) and endometrial cancer (RR = 23.8, CI 6.4-61.0). The relative risk of mutation-negative cases was 2.8 (CI 1.7-4.5) for colorectal cancer and 5.4 (CI 2.0-11.7) for endometrial cancer. We recommend that all double primary patients with cancers at these sites should have a genetic evaluation, including molecular analysis for HNPCC where appropriate. (+info)Multiple primary neoplasms refer to the occurrence of more than one primary malignant tumor in an individual, where each tumor is unrelated to the other and originates from separate cells or organs. This differs from metastatic cancer, where a single malignancy spreads to multiple sites in the body. Multiple primary neoplasms can be synchronous (occurring at the same time) or metachronous (occurring at different times). The risk of developing multiple primary neoplasms increases with age and is associated with certain genetic predispositions, environmental factors, and lifestyle choices such as smoking and alcohol consumption.
A "second primary neoplasm" is a distinct, new cancer or malignancy that develops in a person who has already had a previous cancer. It is not a recurrence or metastasis of the original tumor, but rather an independent cancer that arises in a different location or organ system. The development of second primary neoplasms can be influenced by various factors such as genetic predisposition, environmental exposures, and previous treatments like chemotherapy or radiation therapy.
It is important to note that the definition of "second primary neoplasm" may vary slightly depending on the specific source or context. In general medical usage, it refers to a new, separate cancer; however, in some research or clinical settings, there might be more precise criteria for defining and diagnosing second primary neoplasms.
Pulmonary adenomatosis is a rare condition that is characterized by the abnormal growth of benign tumors (adenomas) in the lungs. These tumors are made up of glands and can cause thickening and enlargement of the lung tissue, which can lead to symptoms such as coughing, wheezing, and difficulty breathing. In some cases, pulmonary adenomatosis may also be associated with an increased risk of lung cancer. It is important to note that this condition is different from adenocarcinoma, which is a type of lung cancer that can also arise in the glands of the lungs.
Skin neoplasms refer to abnormal growths or tumors in the skin that can be benign (non-cancerous) or malignant (cancerous). They result from uncontrolled multiplication of skin cells, which can form various types of lesions. These growths may appear as lumps, bumps, sores, patches, or discolored areas on the skin.
Benign skin neoplasms include conditions such as moles, warts, and seborrheic keratoses, while malignant skin neoplasms are primarily classified into melanoma, squamous cell carcinoma, and basal cell carcinoma. These three types of cancerous skin growths are collectively known as non-melanoma skin cancers (NMSCs). Melanoma is the most aggressive and dangerous form of skin cancer, while NMSCs tend to be less invasive but more common.
It's essential to monitor any changes in existing skin lesions or the appearance of new growths and consult a healthcare professional for proper evaluation and treatment if needed.
A germ-line mutation is a genetic change that occurs in the egg or sperm cells (gametes), and thus can be passed down from parents to their offspring. These mutations are present throughout the entire body of the offspring, as they are incorporated into the DNA of every cell during embryonic development.
Germ-line mutations differ from somatic mutations, which occur in other cells of the body that are not involved in reproduction. While somatic mutations can contribute to the development of cancer and other diseases within an individual, they are not passed down to future generations.
It's important to note that germ-line mutations can have significant implications for medical genetics and inherited diseases. For example, if a parent has a germ-line mutation in a gene associated with a particular disease, their offspring may have an increased risk of developing that disease as well.
Li-Fraumeni Syndrome (LFS) is a rare, hereditary cancer predisposition syndrome. It is characterized by a high risk of developing multiple types of cancers throughout an individual's lifetime. The condition is caused by mutations in the TP53 gene, which plays a crucial role in suppressing tumor growth and maintaining genomic stability.
Individuals with Li-Fraumeni Syndrome have an increased risk of developing various malignancies, including:
1. Sarcomas (soft tissue and bone cancers) - most commonly occurring before the age of 45
2. Breast cancer - often diagnosed at a younger age than sporadic cases
3. Leukemias (blood cancers)
4. Brain tumors, particularly gliomas and medulloblastomas
5. Adrenocortical carcinoma (a rare type of cancer affecting the adrenal glands)
6. Other cancers such as lung, melanoma, and gastrointestinal malignancies
Li-Fraumeni Syndrome is typically inherited in an autosomal dominant manner, meaning that a person has a 50% chance of inheriting the mutated gene from an affected parent. However, de novo (new) mutations can also occur, resulting in individuals with LFS who do not have a family history of the condition.
Due to the high risk of cancer development, individuals with Li-Fraumeni Syndrome require close surveillance and early intervention strategies to manage their cancer risk effectively. Regular screenings, such as magnetic resonance imaging (MRI), computerized tomography (CT) scans, and mammograms, are often recommended for early detection and treatment of potential malignancies.
Paget's disease of the nipple, also known as Paget's disease of the breast, is a rare type of cancer that starts in the breast ducts and spreads to the skin of the nipple and areola. The symptoms often include redness, itching, tingling, or burning of the nipple, which can also become flaky, scaly, or crusty. There may also be a discharge from the nipple.
The exact cause of Paget's disease is not known, but it is thought to be associated with underlying breast cancer in about 90% of cases. It is more common in women over the age of 50 and is usually diagnosed through a biopsy of the affected skin. Treatment typically involves removing the affected breast tissue, which may include a mastectomy, followed by radiation therapy.
It's important to note that Paget's disease of the nipple is different from benign paget's disease of the breast, which is a non-cancerous condition that can cause similar symptoms but does not spread to other parts of the body.
Melanoma is defined as a type of cancer that develops from the pigment-containing cells known as melanocytes. It typically occurs in the skin but can rarely occur in other parts of the body, including the eyes and internal organs. Melanoma is characterized by the uncontrolled growth and multiplication of melanocytes, which can form malignant tumors that invade and destroy surrounding tissue.
Melanoma is often caused by exposure to ultraviolet (UV) radiation from the sun or tanning beds, but it can also occur in areas of the body not exposed to the sun. It is more likely to develop in people with fair skin, light hair, and blue or green eyes, but it can affect anyone, regardless of their skin type.
Melanoma can be treated effectively if detected early, but if left untreated, it can spread to other parts of the body and become life-threatening. Treatment options for melanoma include surgery, radiation therapy, chemotherapy, immunotherapy, and targeted therapy, depending on the stage and location of the cancer. Regular skin examinations and self-checks are recommended to detect any changes or abnormalities in moles or other pigmented lesions that may indicate melanoma.
Hereditary neoplastic syndromes refer to genetic disorders that predispose affected individuals to develop tumors or cancers. These syndromes are caused by inherited mutations in specific genes that regulate cell growth and division. As a result, cells may divide and grow uncontrollably, leading to the formation of benign or malignant tumors.
Examples of hereditary neoplastic syndromes include:
1. Hereditary breast and ovarian cancer syndrome (HBOC): This syndrome is caused by mutations in the BRCA1 or BRCA2 genes, which increase the risk of developing breast, ovarian, and other cancers.
2. Lynch syndrome: Also known as hereditary non-polyposis colorectal cancer (HNPCC), this syndrome is caused by mutations in DNA mismatch repair genes, leading to an increased risk of colon, endometrial, and other cancers.
3. Li-Fraumeni syndrome: This syndrome is caused by mutations in the TP53 gene, which increases the risk of developing a wide range of cancers, including breast, brain, and soft tissue sarcomas.
4. Familial adenomatous polyposis (FAP): This syndrome is caused by mutations in the APC gene, leading to the development of numerous colon polyps that can become cancerous if not removed.
5. Neurofibromatosis type 1 (NF1): This syndrome is caused by mutations in the NF1 gene and is characterized by the development of benign tumors called neurofibromas on the nerves and skin.
6. Von Hippel-Lindau disease (VHL): This syndrome is caused by mutations in the VHL gene, leading to an increased risk of developing various types of tumors, including kidney, pancreas, and adrenal gland tumors.
Individuals with hereditary neoplastic syndromes often have a higher risk of developing cancer than the general population, and they may require more frequent screening and surveillance to detect cancers at an early stage when they are more treatable.
Lung neoplasms refer to abnormal growths or tumors in the lung tissue. These tumors can be benign (non-cancerous) or malignant (cancerous). Malignant lung neoplasms are further classified into two main types: small cell lung carcinoma and non-small cell lung carcinoma. Lung neoplasms can cause symptoms such as cough, chest pain, shortness of breath, and weight loss. They are often caused by smoking or exposure to secondhand smoke, but can also occur due to genetic factors, radiation exposure, and other environmental carcinogens. Early detection and treatment of lung neoplasms is crucial for improving outcomes and survival rates.
Gastrointestinal (GI) neoplasms refer to abnormal growths in the gastrointestinal tract, which can be benign or malignant. The gastrointestinal tract includes the mouth, esophagus, stomach, small intestine, large intestine, rectum, and anus.
Benign neoplasms are non-cancerous growths that do not invade nearby tissues or spread to other parts of the body. They can sometimes be removed completely and may not cause any further health problems.
Malignant neoplasms, on the other hand, are cancerous growths that can invade nearby tissues and organs and spread to other parts of the body through the bloodstream or lymphatic system. These types of neoplasms can be life-threatening if not diagnosed and treated promptly.
GI neoplasms can cause various symptoms, including abdominal pain, bloating, changes in bowel habits, nausea, vomiting, weight loss, and anemia. The specific symptoms may depend on the location and size of the neoplasm.
There are many types of GI neoplasms, including adenocarcinomas, gastrointestinal stromal tumors (GISTs), lymphomas, and neuroendocrine tumors. The diagnosis of GI neoplasms typically involves a combination of medical history, physical examination, imaging studies, and biopsy. Treatment options may include surgery, radiation therapy, chemotherapy, targeted therapy, or immunotherapy.
p16, also known as CDKN2A, is a tumor suppressor gene that encodes the protein p16INK4a. This protein plays a crucial role in regulating the cell cycle by inhibiting the activity of cyclin-dependent kinases (CDKs) 4 and 6, which are essential for the progression from G1 to S phase.
The p16 gene is located on chromosome 9p21 and is often inactivated or deleted in various types of cancer, including lung, breast, and head and neck cancers. Inactivation of the p16 gene leads to uncontrolled cell growth and division, which can contribute to tumor development and progression.
Therefore, the p16 gene is an important tumor suppressor gene that helps prevent cancer by regulating cell growth and division.
Soft tissue neoplasms refer to abnormal growths or tumors that develop in the soft tissues of the body. Soft tissues include muscles, tendons, ligaments, fascia, nerves, blood vessels, fat, and synovial membranes (the thin layer of cells that line joints and tendons). Neoplasms can be benign (non-cancerous) or malignant (cancerous), and their behavior and potential for spread depend on the specific type of neoplasm.
Benign soft tissue neoplasms are typically slow-growing, well-circumscribed, and rarely spread to other parts of the body. They can often be removed surgically with a low risk of recurrence. Examples of benign soft tissue neoplasms include lipomas (fat tumors), schwannomas (nerve sheath tumors), and hemangiomas (blood vessel tumors).
Malignant soft tissue neoplasms, on the other hand, can grow rapidly, invade surrounding tissues, and may metastasize (spread) to distant parts of the body. They are often more difficult to treat than benign neoplasms and require a multidisciplinary approach, including surgery, radiation therapy, and chemotherapy. Examples of malignant soft tissue neoplasms include sarcomas, such as rhabdomyosarcoma (arising from skeletal muscle), leiomyosarcoma (arising from smooth muscle), and angiosarcoma (arising from blood vessels).
It is important to note that soft tissue neoplasms can occur in any part of the body, and their diagnosis and treatment require a thorough evaluation by a healthcare professional with expertise in this area.
p53 is a tumor suppressor gene that encodes a protein responsible for controlling cell growth and division. The p53 protein plays a crucial role in preventing the development of cancer by regulating the cell cycle and activating DNA repair processes when genetic damage is detected. If the damage is too severe to be repaired, p53 can trigger apoptosis, or programmed cell death, to prevent the propagation of potentially cancerous cells. Mutations in the TP53 gene, which encodes the p53 protein, are among the most common genetic alterations found in human cancers and are often associated with a poor prognosis.
Osteosarcoma is defined as a type of cancerous tumor that arises from the cells that form bones (osteoblasts). It's the most common primary bone cancer, and it typically develops in the long bones of the body, such as the arms or legs, near the growth plates. Osteosarcoma can metastasize (spread) to other parts of the body, including the lungs, making it a highly malignant form of cancer. Symptoms may include bone pain, swelling, and fractures. Treatment usually involves a combination of surgery, chemotherapy, and/or radiation therapy.
Breast neoplasms refer to abnormal growths in the breast tissue that can be benign or malignant. Benign breast neoplasms are non-cancerous tumors or growths, while malignant breast neoplasms are cancerous tumors that can invade surrounding tissues and spread to other parts of the body.
Breast neoplasms can arise from different types of cells in the breast, including milk ducts, milk sacs (lobules), or connective tissue. The most common type of breast cancer is ductal carcinoma, which starts in the milk ducts and can spread to other parts of the breast and nearby structures.
Breast neoplasms are usually detected through screening methods such as mammography, ultrasound, or MRI, or through self-examination or clinical examination. Treatment options for breast neoplasms depend on several factors, including the type and stage of the tumor, the patient's age and overall health, and personal preferences. Treatment may include surgery, radiation therapy, chemotherapy, hormone therapy, or targeted therapy.
A registry in the context of medicine is a collection or database of standardized information about individuals who share a certain condition or attribute, such as a disease, treatment, exposure, or demographic group. These registries are used for various purposes, including:
* Monitoring and tracking the natural history of diseases and conditions
* Evaluating the safety and effectiveness of medical treatments and interventions
* Conducting research and generating hypotheses for further study
* Providing information to patients, clinicians, and researchers
* Informing public health policy and decision-making
Registries can be established for a wide range of purposes, including disease-specific registries (such as cancer or diabetes registries), procedure-specific registries (such as joint replacement or cardiac surgery registries), and population-based registries (such as birth defects or cancer registries). Data collected in registries may include demographic information, clinical data, laboratory results, treatment details, and outcomes.
Registries can be maintained by a variety of organizations, including hospitals, clinics, academic medical centers, professional societies, government agencies, and industry. Participation in registries is often voluntary, although some registries may require informed consent from participants. Data collected in registries are typically de-identified to protect the privacy of individuals.
Sarcoma is a type of cancer that develops from certain types of connective tissue (such as muscle, fat, fibrous tissue, blood vessels, or nerves) found throughout the body. It can occur in any part of the body, but it most commonly occurs in the arms, legs, chest, and abdomen.
Sarcomas are classified into two main groups: bone sarcomas and soft tissue sarcomas. Bone sarcomas develop in the bones, while soft tissue sarcomas develop in the soft tissues of the body, such as muscles, tendons, ligaments, fat, blood vessels, and nerves.
Sarcomas can be further classified into many subtypes based on their specific characteristics, such as the type of tissue they originate from, their genetic makeup, and their appearance under a microscope. The different subtypes of sarcoma have varying symptoms, prognoses, and treatment options.
Overall, sarcomas are relatively rare cancers, accounting for less than 1% of all cancer diagnoses in the United States each year. However, they can be aggressive and may require intensive treatment, such as surgery, radiation therapy, and chemotherapy.
Colonic neoplasms refer to abnormal growths in the large intestine, also known as the colon. These growths can be benign (non-cancerous) or malignant (cancerous). The two most common types of colonic neoplasms are adenomas and carcinomas.
Adenomas are benign tumors that can develop into cancer over time if left untreated. They are often found during routine colonoscopies and can be removed during the procedure.
Carcinomas, on the other hand, are malignant tumors that invade surrounding tissues and can spread to other parts of the body. Colorectal cancer is the third leading cause of cancer-related deaths in the United States, and colonic neoplasms are a significant risk factor for developing this type of cancer.
Regular screenings for colonic neoplasms are recommended for individuals over the age of 50 or those with a family history of colorectal cancer or other risk factors. Early detection and removal of colonic neoplasms can significantly reduce the risk of developing colorectal cancer.
I must clarify that the term "pedigree" is not typically used in medical definitions. Instead, it is often employed in genetics and breeding, where it refers to the recorded ancestry of an individual or a family, tracing the inheritance of specific traits or diseases. In human genetics, a pedigree can help illustrate the pattern of genetic inheritance in families over multiple generations. However, it is not a medical term with a specific clinical definition.
DNA Mutational Analysis is a laboratory test used to identify genetic variations or changes (mutations) in the DNA sequence of a gene. This type of analysis can be used to diagnose genetic disorders, predict the risk of developing certain diseases, determine the most effective treatment for cancer, or assess the likelihood of passing on an inherited condition to offspring.
The test involves extracting DNA from a patient's sample (such as blood, saliva, or tissue), amplifying specific regions of interest using polymerase chain reaction (PCR), and then sequencing those regions to determine the precise order of nucleotide bases in the DNA molecule. The resulting sequence is then compared to reference sequences to identify any variations or mutations that may be present.
DNA Mutational Analysis can detect a wide range of genetic changes, including single-nucleotide polymorphisms (SNPs), insertions, deletions, duplications, and rearrangements. The test is often used in conjunction with other diagnostic tests and clinical evaluations to provide a comprehensive assessment of a patient's genetic profile.
It is important to note that not all mutations are pathogenic or associated with disease, and the interpretation of DNA Mutational Analysis results requires careful consideration of the patient's medical history, family history, and other relevant factors.
Genetic predisposition to disease refers to an increased susceptibility or vulnerability to develop a particular illness or condition due to inheriting specific genetic variations or mutations from one's parents. These genetic factors can make it more likely for an individual to develop a certain disease, but it does not guarantee that the person will definitely get the disease. Environmental factors, lifestyle choices, and interactions between genes also play crucial roles in determining if a genetically predisposed person will actually develop the disease. It is essential to understand that having a genetic predisposition only implies a higher risk, not an inevitable outcome.
Head and neck neoplasms refer to abnormal growths or tumors in the head and neck region, which can be benign (non-cancerous) or malignant (cancerous). These tumors can develop in various sites, including the oral cavity, nasopharynx, oropharynx, larynx, hypopharynx, paranasal sinuses, salivary glands, and thyroid gland.
Benign neoplasms are slow-growing and generally do not spread to other parts of the body. However, they can still cause problems if they grow large enough to press on surrounding tissues or structures. Malignant neoplasms, on the other hand, can invade nearby tissues and organs and may also metastasize (spread) to other parts of the body.
Head and neck neoplasms can have various symptoms depending on their location and size. Common symptoms include difficulty swallowing, speaking, or breathing; pain in the mouth, throat, or ears; persistent coughing or hoarseness; and swelling or lumps in the neck or face. Early detection and treatment of head and neck neoplasms are crucial for improving outcomes and reducing the risk of complications.
Squamous cell carcinoma is a type of skin cancer that begins in the squamous cells, which are flat, thin cells that form the outer layer of the skin (epidermis). It commonly occurs on sun-exposed areas such as the face, ears, lips, and backs of the hands. Squamous cell carcinoma can also develop in other areas of the body including the mouth, lungs, and cervix.
This type of cancer usually develops slowly and may appear as a rough or scaly patch of skin, a red, firm nodule, or a sore or ulcer that doesn't heal. While squamous cell carcinoma is not as aggressive as some other types of cancer, it can metastasize (spread) to other parts of the body if left untreated, making early detection and treatment important.
Risk factors for developing squamous cell carcinoma include prolonged exposure to ultraviolet (UV) radiation from the sun or tanning beds, fair skin, a history of sunburns, a weakened immune system, and older age. Prevention measures include protecting your skin from the sun by wearing protective clothing, using a broad-spectrum sunscreen with an SPF of at least 30, avoiding tanning beds, and getting regular skin examinations.
Pancreatic neoplasms refer to abnormal growths in the pancreas that can be benign or malignant. The pancreas is a gland located behind the stomach that produces hormones and digestive enzymes. Pancreatic neoplasms can interfere with the normal functioning of the pancreas, leading to various health complications.
Benign pancreatic neoplasms are non-cancerous growths that do not spread to other parts of the body. They are usually removed through surgery to prevent any potential complications, such as blocking the bile duct or causing pain.
Malignant pancreatic neoplasms, also known as pancreatic cancer, are cancerous growths that can invade and destroy surrounding tissues and organs. They can also spread (metastasize) to other parts of the body, such as the liver, lungs, or bones. Pancreatic cancer is often aggressive and difficult to treat, with a poor prognosis.
There are several types of pancreatic neoplasms, including adenocarcinomas, neuroendocrine tumors, solid pseudopapillary neoplasms, and cystic neoplasms. The specific type of neoplasm is determined through various diagnostic tests, such as imaging studies, biopsies, and blood tests. Treatment options depend on the type, stage, and location of the neoplasm, as well as the patient's overall health and preferences.
In the context of medicine, risk is the probability or likelihood of an adverse health effect or the occurrence of a negative event related to treatment or exposure to certain hazards. It is usually expressed as a ratio or percentage and can be influenced by various factors such as age, gender, lifestyle, genetics, and environmental conditions. Risk assessment involves identifying, quantifying, and prioritizing risks to make informed decisions about prevention, mitigation, or treatment strategies.
Adenocarcinoma is a type of cancer that arises from glandular epithelial cells. These cells line the inside of many internal organs, including the breasts, prostate, colon, and lungs. Adenocarcinomas can occur in any of these organs, as well as in other locations where glands are present.
The term "adenocarcinoma" is used to describe a cancer that has features of glandular tissue, such as mucus-secreting cells or cells that produce hormones. These cancers often form glandular structures within the tumor mass and may produce mucus or other substances.
Adenocarcinomas are typically slow-growing and tend to spread (metastasize) to other parts of the body through the lymphatic system or bloodstream. They can be treated with surgery, radiation therapy, chemotherapy, targeted therapy, or a combination of these treatments. The prognosis for adenocarcinoma depends on several factors, including the location and stage of the cancer, as well as the patient's overall health and age.
In epidemiology, the incidence of a disease is defined as the number of new cases of that disease within a specific population over a certain period of time. It is typically expressed as a rate, with the number of new cases in the numerator and the size of the population at risk in the denominator. Incidence provides information about the risk of developing a disease during a given time period and can be used to compare disease rates between different populations or to monitor trends in disease occurrence over time.
Neoplasms are abnormal growths of cells or tissues in the body that serve no physiological function. They can be benign (non-cancerous) or malignant (cancerous). Benign neoplasms are typically slow growing and do not spread to other parts of the body, while malignant neoplasms are aggressive, invasive, and can metastasize to distant sites.
Neoplasms occur when there is a dysregulation in the normal process of cell division and differentiation, leading to uncontrolled growth and accumulation of cells. This can result from genetic mutations or other factors such as viral infections, environmental exposures, or hormonal imbalances.
Neoplasms can develop in any organ or tissue of the body and can cause various symptoms depending on their size, location, and type. Treatment options for neoplasms include surgery, radiation therapy, chemotherapy, immunotherapy, and targeted therapy, among others.
Prognosis is a medical term that refers to the prediction of the likely outcome or course of a disease, including the chances of recovery or recurrence, based on the patient's symptoms, medical history, physical examination, and diagnostic tests. It is an important aspect of clinical decision-making and patient communication, as it helps doctors and patients make informed decisions about treatment options, set realistic expectations, and plan for future care.
Prognosis can be expressed in various ways, such as percentages, categories (e.g., good, fair, poor), or survival rates, depending on the nature of the disease and the available evidence. However, it is important to note that prognosis is not an exact science and may vary depending on individual factors, such as age, overall health status, and response to treatment. Therefore, it should be used as a guide rather than a definitive forecast.
A mutation is a permanent change in the DNA sequence of an organism's genome. Mutations can occur spontaneously or be caused by environmental factors such as exposure to radiation, chemicals, or viruses. They may have various effects on the organism, ranging from benign to harmful, depending on where they occur and whether they alter the function of essential proteins. In some cases, mutations can increase an individual's susceptibility to certain diseases or disorders, while in others, they may confer a survival advantage. Mutations are the driving force behind evolution, as they introduce new genetic variability into populations, which can then be acted upon by natural selection.
Neoplasm staging is a systematic process used in medicine to describe the extent of spread of a cancer, including the size and location of the original (primary) tumor and whether it has metastasized (spread) to other parts of the body. The most widely accepted system for this purpose is the TNM classification system developed by the American Joint Committee on Cancer (AJCC) and the Union for International Cancer Control (UICC).
In this system, T stands for tumor, and it describes the size and extent of the primary tumor. N stands for nodes, and it indicates whether the cancer has spread to nearby lymph nodes. M stands for metastasis, and it shows whether the cancer has spread to distant parts of the body.
Each letter is followed by a number that provides more details about the extent of the disease. For example, a T1N0M0 cancer means that the primary tumor is small and has not spread to nearby lymph nodes or distant sites. The higher the numbers, the more advanced the cancer.
Staging helps doctors determine the most appropriate treatment for each patient and estimate the patient's prognosis. It is an essential tool for communication among members of the healthcare team and for comparing outcomes of treatments in clinical trials.
Neoplasms: Neoplasms refer to abnormal growths of tissue that can be benign (non-cancerous) or malignant (cancerous). They occur when the normal control mechanisms that regulate cell growth and division are disrupted, leading to uncontrolled cell proliferation.
Cystic Neoplasms: Cystic neoplasms are tumors that contain fluid-filled sacs or cysts. These tumors can be benign or malignant and can occur in various organs of the body, including the pancreas, ovary, and liver.
Mucinous Neoplasms: Mucinous neoplasms are a type of cystic neoplasm that is characterized by the production of mucin, a gel-like substance produced by certain types of cells. These tumors can occur in various organs, including the ovary, pancreas, and colon. Mucinous neoplasms can be benign or malignant, and malignant forms are often aggressive and have a poor prognosis.
Serous Neoplasms: Serous neoplasms are another type of cystic neoplasm that is characterized by the production of serous fluid, which is a thin, watery fluid. These tumors commonly occur in the ovary and can be benign or malignant. Malignant serous neoplasms are often aggressive and have a poor prognosis.
In summary, neoplasms refer to abnormal tissue growths that can be benign or malignant. Cystic neoplasms contain fluid-filled sacs and can occur in various organs of the body. Mucinous neoplasms produce a gel-like substance called mucin and can also occur in various organs, while serous neoplasms produce thin, watery fluid and commonly occur in the ovary. Both mucinous and serous neoplasms can be benign or malignant, with malignant forms often being aggressive and having a poor prognosis.
Exons are the coding regions of DNA that remain in the mature, processed mRNA after the removal of non-coding intronic sequences during RNA splicing. These exons contain the information necessary to encode proteins, as they specify the sequence of amino acids within a polypeptide chain. The arrangement and order of exons can vary between different genes and even between different versions of the same gene (alternative splicing), allowing for the generation of multiple protein isoforms from a single gene. This complexity in exon structure and usage significantly contributes to the diversity and functionality of the proteome.
Retrospective studies, also known as retrospective research or looking back studies, are a type of observational study that examines data from the past to draw conclusions about possible causal relationships between risk factors and outcomes. In these studies, researchers analyze existing records, medical charts, or previously collected data to test a hypothesis or answer a specific research question.
Retrospective studies can be useful for generating hypotheses and identifying trends, but they have limitations compared to prospective studies, which follow participants forward in time from exposure to outcome. Retrospective studies are subject to biases such as recall bias, selection bias, and information bias, which can affect the validity of the results. Therefore, retrospective studies should be interpreted with caution and used primarily to generate hypotheses for further testing in prospective studies.
Medical Definition:
"Risk factors" are any attribute, characteristic or exposure of an individual that increases the likelihood of developing a disease or injury. They can be divided into modifiable and non-modifiable risk factors. Modifiable risk factors are those that can be changed through lifestyle choices or medical treatment, while non-modifiable risk factors are inherent traits such as age, gender, or genetic predisposition. Examples of modifiable risk factors include smoking, alcohol consumption, physical inactivity, and unhealthy diet, while non-modifiable risk factors include age, sex, and family history. It is important to note that having a risk factor does not guarantee that a person will develop the disease, but rather indicates an increased susceptibility.
Tumor suppressor protein p53, also known as p53 or tumor protein p53, is a nuclear phosphoprotein that plays a crucial role in preventing cancer development and maintaining genomic stability. It does so by regulating the cell cycle and acting as a transcription factor for various genes involved in apoptosis (programmed cell death), DNA repair, and cell senescence (permanent cell growth arrest).
In response to cellular stress, such as DNA damage or oncogene activation, p53 becomes activated and accumulates in the nucleus. Activated p53 can then bind to specific DNA sequences and promote the transcription of target genes that help prevent the proliferation of potentially cancerous cells. These targets include genes involved in cell cycle arrest (e.g., CDKN1A/p21), apoptosis (e.g., BAX, PUMA), and DNA repair (e.g., GADD45).
Mutations in the TP53 gene, which encodes p53, are among the most common genetic alterations found in human cancers. These mutations often lead to a loss or reduction of p53's tumor suppressive functions, allowing cancer cells to proliferate uncontrollably and evade apoptosis. As a result, p53 has been referred to as "the guardian of the genome" due to its essential role in preventing tumorigenesis.
Follow-up studies are a type of longitudinal research that involve repeated observations or measurements of the same variables over a period of time, in order to understand their long-term effects or outcomes. In medical context, follow-up studies are often used to evaluate the safety and efficacy of medical treatments, interventions, or procedures.
In a typical follow-up study, a group of individuals (called a cohort) who have received a particular treatment or intervention are identified and then followed over time through periodic assessments or data collection. The data collected may include information on clinical outcomes, adverse events, changes in symptoms or functional status, and other relevant measures.
The results of follow-up studies can provide important insights into the long-term benefits and risks of medical interventions, as well as help to identify factors that may influence treatment effectiveness or patient outcomes. However, it is important to note that follow-up studies can be subject to various biases and limitations, such as loss to follow-up, recall bias, and changes in clinical practice over time, which must be carefully considered when interpreting the results.
In the field of medicine, "time factors" refer to the duration of symptoms or time elapsed since the onset of a medical condition, which can have significant implications for diagnosis and treatment. Understanding time factors is crucial in determining the progression of a disease, evaluating the effectiveness of treatments, and making critical decisions regarding patient care.
For example, in stroke management, "time is brain," meaning that rapid intervention within a specific time frame (usually within 4.5 hours) is essential to administering tissue plasminogen activator (tPA), a clot-busting drug that can minimize brain damage and improve patient outcomes. Similarly, in trauma care, the "golden hour" concept emphasizes the importance of providing definitive care within the first 60 minutes after injury to increase survival rates and reduce morbidity.
Time factors also play a role in monitoring the progression of chronic conditions like diabetes or heart disease, where regular follow-ups and assessments help determine appropriate treatment adjustments and prevent complications. In infectious diseases, time factors are crucial for initiating antibiotic therapy and identifying potential outbreaks to control their spread.
Overall, "time factors" encompass the significance of recognizing and acting promptly in various medical scenarios to optimize patient outcomes and provide effective care.
Kidney neoplasms refer to abnormal growths or tumors in the kidney tissues that can be benign (non-cancerous) or malignant (cancerous). These growths can originate from various types of kidney cells, including the renal tubules, glomeruli, and the renal pelvis.
Malignant kidney neoplasms are also known as kidney cancers, with renal cell carcinoma being the most common type. Benign kidney neoplasms include renal adenomas, oncocytomas, and angiomyolipomas. While benign neoplasms are generally not life-threatening, they can still cause problems if they grow large enough to compromise kidney function or if they undergo malignant transformation.
Early detection and appropriate management of kidney neoplasms are crucial for improving patient outcomes and overall prognosis. Regular medical check-ups, imaging studies, and urinalysis can help in the early identification of these growths, allowing for timely intervention and treatment.
 Lymphoid neoplasms with plasmablastic differentiation
Lymphoid neoplasms with plasmablastic differentiation
Myeloproliferative neoplasm
Canine histiocytic diseases
List of ICD-9 codes 140-239: neoplasms
Frederick Pei Li
Primary myelofibrosis
Lindsay Morton
Granular cell tumor
Mouse models of breast cancer metastasis
Ollier disease
Mucinous neoplasm
Ameloblastoma
C97
Gastrinoma
International Classification of Diseases for Oncology
NOL3
List of cancer types
Li-Fraumeni syndrome
Colorectal polyp
Bone tumor
Low-grade fibromyxoid sarcoma
Plasmacytoma
Follicular lymphoma
Lymphoma
Gardner's syndrome
Folliculin
List of skin conditions
Neuroendocrine tumor
Syndecan 1
Reticuloendotheliosis virus
 Analysis of polymorphisms in genes associated with the FA/BRCA pathway in three patients with multiple primary malignant...
Analysis of polymorphisms in genes associated with the FA/BRCA pathway in three patients with multiple primary malignant...
 CML Following Treatment for Primary Neoplasms
CML Following Treatment for Primary Neoplasms
 Category C - Diseases
Category C - Diseases
 Preventing Chronic Disease | Test of an Electronic Program to Query Clinicians About Nonspecific Causes Reported for Pneumonia...
Preventing Chronic Disease | Test of an Electronic Program to Query Clinicians About Nonspecific Causes Reported for Pneumonia...
NIH Guide: AGING AND OLD AGE AS RISK FACTORS FOR MULTIPLE PRIMARY TUMORS
The incidence of multiple primary malignant neoplasms increases with age, reflecting - Apoptosis in amphibian organs
Biomarkers Search
Prognostic factors of early gastric cancer--results of long-term follow-up and analysis of recurrent cases
Microcarcinoma in the prostate: its association with duct-acinar dysplasia
Early Release - Case Report of Nasal Rhinosporidiosis in South Africa - Volume 30, Number 4-April 2024 - Emerging Infectious...
 Multiple hepatic adenomas and a hepatocellular carcinoma in a man on oral methyl testosterone for eleven years - PubMed
Multiple hepatic adenomas and a hepatocellular carcinoma in a man on oral methyl testosterone for eleven years - PubMed
 Revision History for the Hematopoietic Project - SEER Registrars
Revision History for the Hematopoietic Project - SEER Registrars
Lymphoid neoplasms with plasmablastic differentiation - Wikipedia
 Molecular Vision: ETS-1 and ETS-2 are upregulated in a
transgenic mouse model of pigmented ocular neoplasm
Molecular Vision: ETS-1 and ETS-2 are upregulated in a
transgenic mouse model of pigmented ocular neoplasm
 Biblio | Linus Pauling Institute | Oregon State University
Biblio | Linus Pauling Institute | Oregon State University
Meningioma: Practice Essentials, Background, Pathophysiology
NIH VideoCast - NCI Science Writer's Seminar on Second Cancers
 Bevillinger fra Overlægerådets forskningsfond
Bevillinger fra Overlægerådets forskningsfond
HuGE Navigator|Genopedia|PHGKB
IndexCat
 Brown Tumor of the Maxilla Revealing Primary Hyperparathyroidism
Brown Tumor of the Maxilla Revealing Primary Hyperparathyroidism
 A False Positive I-131 Metastatic Survey Caused by Radioactive Iodine Uptake by a Benign Thymic Cyst
A False Positive I-131 Metastatic Survey Caused by Radioactive Iodine Uptake by a Benign Thymic Cyst
 Linet, Martha 2022 - Office of NIH History and Stetten Museum
Linet, Martha 2022 - Office of NIH History and Stetten Museum
Glossary | Daniel Nathans - Profiles in Science
Metastatic renal cell carcinoma to the small bowel 6 years postnephrectomy | BMJ Case Reports
 OC treatment for my dear Aunt - Cancer Survivors Network
OC treatment for my dear Aunt - Cancer Survivors Network
 C62542|Tooth Crowding|create|29-SEP-06|(null)|(null
C62542|Tooth Crowding|create|29-SEP-06|(null)|(null
Myeloma11
- 2) Plasmablastic plasma cell lymphoma or plasmablastic plasmacytoma: A lymphoid neoplasm that disseminates widely like the plasma cell lesions in multiple myeloma or is localized like the plasma cell lesions in plasmacytoma. (wikipedia.org)
- Multiple myeloma (MM) , also known as plasma cell myeloma , is a multifocal proliferation of plasma cells based in the bone marrow . (radiopaedia.org)
- Multiple myeloma remains incurable. (radiopaedia.org)
- Multiple myeloma accounts for one of the 'M's in the popular mnemonic for lucent bone lesions FEGNOMASHIC . (radiopaedia.org)
- As per the WHO classification of tumors of hematopoietic and lymphoid tissues , multiple myeloma is called plasma cell myeloma 14 . (radiopaedia.org)
- Smoldering multiple myeloma refers to a form that falls on the spectrum between monoclonal gammopathy of unknown significance (MGUS) and active multiple myeloma. (radiopaedia.org)
- Patients are asymptomatic, with worse biochemistry than MGUS but without the end-organ damage of active multiple myeloma 9 . (radiopaedia.org)
- Multiple myeloma and osteosarcoma combined account for ~50% of all primary bone malignancies 7 . (radiopaedia.org)
- 1 B cell neoplasms other than multiple myeloma including non-Hodgkin's lymphomas, and acute and chronic leukaemias might also exhibit lytic bone lesions, hypercalcaemia, and monoclonal gammopathy via the particular actions of interleukin (IL-1), IL-6, or tumour necrosis factor-α secreted by the neoplastic B cell clone, but not reported previously secondary to a primary cerebral lymphoma. (bmj.com)
- 5. Which of the following is a characteristic feature of multiple myeloma? (medicalbiochemist.com)
- Multiple Myeloma Multiple myeloma is a cancer of plasma cells that produce monoclonal immunoglobulin and invade and destroy adjacent bone tissue. (msdmanuals.com)
Tumors17
- Choroid plexus neoplasms are rare, intraventricular, primary central nervous system (CNS) tumors derived from choroid plexus epithelium that are seen predominantly in children. (medscape.com)
- [ 2 , 3 ] In adults, they account for less than 1% of primary intracranial neoplasms, whereas choroid plexus tumors represent up to 5% of pediatric brain tumors, and up to 20% of those arising in children aged 1 year and younger. (medscape.com)
- 3. Torre D. Multiple sebaceous tumors. (meduniver.com)
- Incidence of primary large bowel lymphomas comprises only 0.2-0.6% of large bowel malignant tumors ( 3 ). (frontiersin.org)
- The frequency of meningiomas in Africa is nearly 30% of all primary intracranial tumors. (medscape.com)
- Most primary brain tumors are solitary, but multiple primary brain tumors have been reported. (vin.com)
- Secondary or metastatic tumors appear to be less common and may result from local extension (e.g., nasal adenocarcinoma) or metastases from primary tumors elsewhere. (vin.com)
- Primary tumors other than meningiomas appear to be less common in cats than in dogs. (vin.com)
- Primary brain tumors originate from cells normally found within the brain and meninges. (vin.com)
- Secondary tumors are metastasis from a primary tumor located outside the nervous system, or occur by local invasion from adjacent non- neural tissues (e.g., bone). (vin.com)
- Pituitary gland neoplasms and tumors arising from cranial nerves are considered secondary brain tumors. (vin.com)
- Primary brain tumors often are slow growing and the brain adapts to the slow increase in ICP. (vin.com)
- Biochemical signs and severity of symptoms of primary hyperparathyroidism (pHPT) differ among patients, and little is known of any coupling of clinical characteristics of nonfamilial pHPT to genetic abnormalities in the parathyroid tumors. (lu.se)
- Hemangiosarcomas are locally invasive and multicentric ( having two or more primary tumors ). (ivis.org)
- The focused ultrasound assessment with sonograms in trauma (FAST) revealed multiple tumors in the heart which were then confirmed in echocardiographic examination performed by a veterinary cardiologist. (biomedcentral.com)
- Heart tumors (HT) are uncommon in companion animals, accounting for roughly 0.2% of all neoplasms. (biomedcentral.com)
- For multiple neoplasms of the same site that are not contiguous, such as tumors in different quadrants of the same breast, codes for each site should be assigned. (icd10data.com)
Benign1
- Malignant neoplasms show a greater degree of anaplasia and have the properties of invasion and metastasis, compared to benign neoplasms . (lookformedical.com)
Brain neoplasms1
- Gliomas are the most common primary brain neoplasms. (medscimonit.com)
Myeloproliferative Neoplasms2
- Patients with underlying hypercoagulable states, most frequently myeloproliferative neoplasms, are at highest risk for primary Budd-Chiari syndrome, and multiple genes have been associated. (logicalimages.com)
- 10. Which of the following is a common finding in myeloproliferative neoplasms (MPNs)? (medicalbiochemist.com)
Melanoma3
- Multiple malignant melanocytic lesions developed in a 54-year-old man 4 years after a primary malignant melanoma (Clark level IV) had been excised and 2 months after taking L-Dopa for Parkinsonism. (nih.gov)
- Choroidal melanoma is the most common primary malignant ocular tumor in human adults. (molvis.org)
- We have studied the transgenic mouse strain, Tyrp-1-TAg, to try to gain insight into possible molecular mechanisms common to pigmented ocular neoplasms occurring spontaneously in the eyes of these mice and human choroidal melanoma. (molvis.org)
Metastasis1
- Lee V, Gessler D, Cataltepe O. Case report: cranial angiosarcoma with multiple hemorrhagic brain metastasis in a child. (umassmed.edu)
Carcinoma2
- Transarterial radioembolization (TARE) with yttrium 90 is increasingly utilized for the treatment of hepatic neoplasms, whether primary (particularly hepatocellular carcinoma [HCC]) or metastatic (particularly colorectal). (thieme-connect.com)
- They also show that families with the CDKN2A 113insArg mutation have an increased risk not only of multiple melanomas and pancreatic carcinoma but also of breast cancer. (lu.se)
Lymphoid6
- Lymphoid neoplasms with plasmablastic differentiation were classified by the World Health Organization, 2017 as a sub-grouping of several distinct but rare lymphomas in which the malignant cells are B-cell lymphocytes that have become plasmablasts, i.e. immature plasma cells. (wikipedia.org)
- Due to their malignant nature, however, the plasmablasts in lymphoid neoplasms with plasmablastic differentiation do not mature into plasma cells or form antibodies but rather uncontrollably proliferate in and damage various tissues and organs. (wikipedia.org)
- The lymphoid neoplasms with plasmacytic differentiation are: 1) Plasmablastic lymphoma: The most common of these lymphoid neoplasms. (wikipedia.org)
- 6) Human herpesvirus 8-positive diffuse large B-cell lymphoma, not otherwise specified: This lymphoid neoplasm usually arises from the lymphoproliferative disease, idiopathic multicentric Castleman disease. (wikipedia.org)
- Except for human herpesvirus 8-positive diffuse large B-cell lymphoma, not otherwise specified, these lymphoid neoplasms are often associated with Epstein-Barr virus infection of the malignant plasmablastic cells. (wikipedia.org)
- In cases so infected, the lymphoid neoplasm may result, at least in part, from this viral infection and therefore can be considered as examples of the Epstein-Barr virus-associated lymphoproliferative diseases. (wikipedia.org)
Malignant neoplasm1
- A primary malignant neoplasm that overlaps two or more contiguous (next to each other) sites should be classified to the subcategory/code .8 ('overlapping lesion'), unless the combination is specifically indexed elsewhere. (icd10data.com)
Growths of tissue1
- Abnormal growths of tissue that follow a previous neoplasm but are not metastases of the latter. (lookformedical.com)
Diagnosis7
- Early diagnosis of primary intestinal NK/T cell lymphoma is frequently difficult. (frontiersin.org)
- Herein we report a case with unilateral abducens nerve palsy as initial symptom in the primary sphenoidal sinus ENKL and investigated the clinical feature of the diagnosis and therapy. (hindawi.com)
- Staging procedures including CT of the abdomen and pelvis, bilateral bone marrow aspiration, and biopsies were within normal limits precluding the diagnosis of primary cerebral lymphoma. (bmj.com)
- 2007) The utility of Pax-5 immunohistochemistry in the diagnosis of undifferentiated malignant neoplasms Mod. (roche.com)
- BACKGROUND: Spinal metastases are being diagnosed more frequently because of increasing life expectancies and advances in the diagnosis and therapy of primary tumours. (iospress.com)
- The occurrence of this tumor in the heart has been described only in a few publications in dogs, and such a multiple heart RMS as presented below is an extremely uncommon diagnosis not only in veterinary but also in human medicine. (biomedcentral.com)
- If the features of anxiety that are seen are not typical for a primary anxiety disorder, and there is a medical condition present, this is an indication that anxiety due to another medical condition may be an appropriate diagnosis. (theravive.com)
Lymphoma4
- Extranodal NK/T cell lymphoma is a rare non-Hodgkin lymphoma mainly involving the upper aerodigestive tract, even rarer is primary extranasal disease involving the intestine. (frontiersin.org)
- We present a case of primary intestinal NK/T cell lymphoma with diagnostic challenge, which eventually developed into multiple intestinal perforations. (frontiersin.org)
- Primary cerebral lymphoma is a unique and infrequent CNS malignancy in which the B lymphocyte subtype constitutes most cases. (bmj.com)
- 2 We describe an unusual presentation of a B cell primary cerebral lymphoma mimicking a plasma cell dyscrasia. (bmj.com)
Etiology1
- Clinicians should be careful to exclude other etiologies of liver failure that can predispose patients to developing hepatic venous outflow tract obstruction that is either nonocclusive or not the primary etiology of the patient's liver failure. (logicalimages.com)
Cancer2
- 0001). Families with breast cancer also had a propensity for multiple melanomas in females, suggesting that a sex-dependent factor may modify the phenotypic expression of CDKN2A alterations. (lu.se)
- Title : The effect of multiple primary rules on population-based cancer survival Personal Author(s) : Weir, Hannah K.;Johnson, Christopher J.;Thompson, Trevor D. (cdc.gov)
Lymphatic system1
- Transfer of a neoplasm from its primary site to lymph nodes or to distant parts of the body by way of the lymphatic system. (lookformedical.com)
Pancreas1
- Malignant neoplasms of ectopic tissue are to be coded to the site mentioned, e.g., ectopic pancreatic malignant neoplasms are coded to pancreas, unspecified ( C25.9 ). (icd10data.com)
Intracranial2
- Choroid plexus neoplasms can produce hydrocephalus and increased intracranial pressure by a number of mechanisms, including obstruction of normal cerebrospinal fluid (CSF) flow, overproduction of CSF by the tumor itself, local expansion of the ventricles, or spontaneous hemorrhage. (medscape.com)
- Meningiomas account for approximately 20% of all primary intracranial neoplasms. (medscape.com)
Secondary5
- Radioembolization with 90 yttrium microspheres: a state-of-the-art brachytherapy treatment for primary and secondary liver malignancies. (thieme-connect.com)
- Synovial chondromatosis occurs as either a primary or a secondary form. (medscape.com)
- Budd-Chiari syndrome is hepatic venous outflow tract obstruction due to either primary vascular occlusion (thrombosis) or secondary occlusion from extrinsic compression (eg, malignancy). (logicalimages.com)
- Examination of cells whether from a primary or secondary site, including fluids aspirated using endoscopes or needles. (who.int)
- It can be present in two forms: primary or secondary. (bvsalud.org)
Chronic2
- Common types of MPNs include chronic myeloid leukemia (CML), polycythemia vera (PV), essential thrombocythemia (ET), and primary myelofibrosis (PMF). (medicalbiochemist.com)
- 1. Which of the following is NOT a primary characteristic feature of chronic myeloid leukemia (CML)? (medicalbiochemist.com)
Malignancies2
- It accounts for 1% of all malignancies and 10-15% of all hematological neoplasms 12,14 . (radiopaedia.org)
- Two cases of multiple primary malignancies (two or more neoplasms without any relationship between them) are presented in this paper. (banglajol.info)
Ovarian1
- 18 With the exception of the ovarian neoplasms, the same carcinomas analyzed for gene expression were also examined for HE4 by immunohistochemistry on tissue microarrays (see below). (nature.com)
Molecular2
- Undoubtedly, advances in molecular biology will allow scientists to determine the exact genomic aberration responsible for each specific neoplasm. (medscape.com)
- Using a combination of molecular dynamics (MD) simulations and small-angle X-ray scattering (SAXS), we discovered an allosteric interface between the SH2 and kinase domain required for Btk activation and to which multiple XLA mutations map. (rcsb.org)
Arises1
- The second neoplasm may have the same or different histological type and can occur in the same or different organs as the previous neoplasm but in all cases arises from an independent oncogenic event. (lookformedical.com)
Histology1
- A review of 155 cases of primary synovial chondromatosis by McCarthy et al identified only four cases of aggressive behavior and chondrosarcomalike histology (one in the elbow and three in the hip). (medscape.com)
Disease2
- Several of the recurrent lesions that showed junctional melanocytic components were considered primary melanomas and it was suggested that L-Dopa was responsible for malignant transformation of nevi and for rapid progression of the disease. (nih.gov)
- The common causes of unilateral abducens nerve palsy are neoplasm and vascular disease in middle-aged people [ 1 ]. (hindawi.com)
Factors2
- Multiple geenetic and environmental factors have been linked to the development of CRC. (mindmeister.com)
- The development of the second neoplasm may or may not be related to the treatment for the previous neoplasm since genetic risk or predisposing factors may actually be the cause. (lookformedical.com)
Hypertension1
- 1 in Europe, hypertension is one of the most common interventions in primary care, and CCBs are a first-line treatment for this. (bmj.com)
MESH1
- Multiple Endocrine Neoplasia Type 2b" is a descriptor in the National Library of Medicine's controlled vocabulary thesaurus, MeSH (Medical Subject Headings) . (umassmed.edu)
Malignancy1
- This association may not be fortuitous and suggests that patients with multiple hamartomas of the perifollicular connective tissue should be examined periodically for intestinal polyps before malignancy develops. (nih.gov)
Metastatic1
- 11 Lee EJ, Chung HW, Jo JH, So Y. Radioembolization for the treatment of primary and metastatic liver cancers. (thieme-connect.com)
Genes3
- Our data show that, in contrast to adult MDS, Ras/MAPK pathway mutations are common in pediatric MDS (45% of primary cohort), while mutations in RNA splicing genes are rare (2% of primary cohort). (nature.com)
- Multiple large cohort studies of adult MDS patients found recurrent mutations in genes important in epigenetic regulation (e.g. (nature.com)
- We show that Ras/MAPK pathway mutations are common in pediatric primary MDS (45%) while mutations in RNA splicing genes are rare (2%), and that germline SAMD9/SAMD9L mutations are present in 17% of primary MDS patients. (nature.com)
Rectum1
- CRC is a neoplasm that develops in the colon or rectum. (mindmeister.com)
Colon5
- Multiple primary carcinomata of the colon duodenum and larynx associated with keratoacanthoma of the face. (meduniver.com)
- Colonoscopy showed multiple irregular ulcers in colon. (frontiersin.org)
- The resected specimen showed multiple perforations of the colon. (frontiersin.org)
- In this paper, we describe a very rare case of ENKTL involving the colon with multiple intestinal perforations. (frontiersin.org)
- A total of three colonoscopes and biopsies were performed for the patient, and the results showed multiple irregular ulcers in the whole colon ( Figure 1 ). (frontiersin.org)
Cranial3
- Multiple cranial nerve deficits or bilateral abducens nerve palsy associated with ENKL have been reported [ 3 ], but isolated unilateral abducens palsy is rarely reported. (hindawi.com)
- Neoplasms involving the brain stem may result in cranial nerve deficits. (vin.com)
- Direct lateral radiography of the skull of the patient, showing multiple punched out lytic lesions of the cranial vault, with no evidence of a periosteal reaction. (bmj.com)